|
Overview
 Even though bunions are a common foot deformity, there are misconceptions about them. Many people may unnecessarily suffer the pain of bunions for years before seeking treatment. A bunion (also referred to as hallux valgus or hallux abducto valgus) is often described as a bump on the side of the big toe. But a bunion is more than that. The visible bump actually reflects changes in the bony framework of the front part of the foot. The big toe leans toward the second toe, rather than pointing straight ahead. This throws the bones out of alignment, producing the bunion?s ?bump.? Bunions are a progressive disorder. They begin with a leaning of the big toe, gradually changing the angle of the bones over the years and slowly producing the characteristic bump, which becomes increasingly prominent. Symptoms usually appear at later stages, although some people never have symptoms. Even though bunions are a common foot deformity, there are misconceptions about them. Many people may unnecessarily suffer the pain of bunions for years before seeking treatment. A bunion (also referred to as hallux valgus or hallux abducto valgus) is often described as a bump on the side of the big toe. But a bunion is more than that. The visible bump actually reflects changes in the bony framework of the front part of the foot. The big toe leans toward the second toe, rather than pointing straight ahead. This throws the bones out of alignment, producing the bunion?s ?bump.? Bunions are a progressive disorder. They begin with a leaning of the big toe, gradually changing the angle of the bones over the years and slowly producing the characteristic bump, which becomes increasingly prominent. Symptoms usually appear at later stages, although some people never have symptoms.Causes Bunions, Corns, and Calluses are all related in that they can each be caused by tight and/or poor fitting footwear. Each can also be caused by the following, footwear that is too narrow and/or too small. Constrictive toe boxes (toe area). Tapered toe boxes can cause bunions and cause them to worsen to the point of needing surgery. Symptoms Corns and calluses may occur on the soles of the feet, in between toes and on the bunion joint. Stiffness can occur at the big toe due to secondary arthritis, this is known as Hallux Rigidus. Other foot conditions can occur such as in growing toenails and in severe cases the bunion joint may have a fluid filled sack called a bursitis. This can be very painful and can become infected. Diagnosis A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen. Non Surgical Treatment Some bunions can be treated without surgery. If you have a bunion, wear shoes that are roomy enough so that they won?t put pressure on it. You can choose to have your shoes stretched out professionally or try cushioning the painful area with protective pads. Orthotics have been shown to help prevent progression of bunions. Oral nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be recommended to reduce pain and inflammation. Applying an ice pack several times a day can also help reduce inflammation and pain. If your bunion progresses to a point where you have difficulty walking or experience pain even with accommodative shoes, surgery may be necessary. 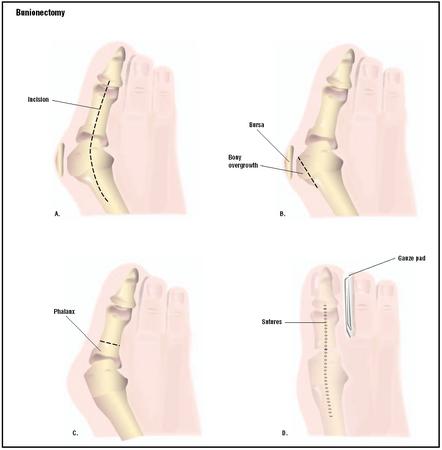 Surgical Treatment Larger bunions often require the surgeon to move the entire bone over (1st metatarsal). This is accomplished by a cut or fusion at the bottom of the bone. The former technique, is called the Lapidus bunionectomy. Additionally, the repositioned bone is held in place with one or two surgical screws. Prevention To help prevent bunions be sure your shoes don't cramp or irritate your toes. Choose shoes with a wide toe box - there should be space between the tip of your longest toe and the end of the shoe. Your shoes should conform to the shape of your feet without squeezing or pressing any part of your foot. Avoid pointy-toed shoes. Overview
Pronation occurs as weight is transferred from the heel to the forefoot and the foot rolls inwards. Or to put it a little more technically; pronation is the movement of the subtalar joint (between the talus and calcaneus) into eversion, dorsi flexion and abduction (turning the sole outwards, upwards and sideways). A certain amount of this is natural but it many people the foot rolls in too much or over pronates.  Causes It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses. Symptoms Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses. Diagnosis At some point you may find the pain to much or become frustrated. So what are you options? Chances are your overpronation has led to some type of injury if there's pain. Your best bet is to consult with someone who knows feet. Start with your pediatrist, chiropodist or chiropractor. They'll be able to diagnose and treat the injury and give you more specific direction to better support your feet. One common intervention is a custom foot orthotic. Giving greater structural support than a typical shoe these shoe inserts can dramatically reduce overpronation.  Non Surgical Treatment When you see the doctor, he or she will likely perform a complete examination of your feet and watch you walk. The doctor will need to take x-rays to determine the cause of your flat feet. In some cases, further imaging may be needed, especially if your symptoms are severe and sudden in nature. Once you are properly diagnosed, your doctor will create an appropriate treatment plan. There are several options to correct overpronation, such as orthotics. In many cases, overpronation can be treated with non-surgical methods and over-the-counter orthotics. In severe cases, however, custom-made orthotics may work better. Orthotics provide arch support and therefore prevent collapse of the arch with weight bearing. They are made of materials such as spongy rubber or hard plastic. Your doctor will also want to examine your footwear to ensure they fit properly and offer enough medial support. Extra support and stability can be achieved with footwear that has a firm heel counter. If you are experiencing pain, you should be able to use over-the-counter pain medications such as ibuprofen to relieve symptoms. Surgical Treatment HyProCure implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%. Overview
If your teen or preteen is complaining of heel pain, it might be Sever?s disease. No need to stress - this isn?t actually a ?disease,? but rather a common type of growing pain that only lasts a few weeks or months and doesn?t leave any long-term damage. Sever?s disease occurs in kids as they hit their adolescent growth spurt, usually between the ages of 8-13 for girls and 10-15 for boys. It?s most common among active kids that run, play basketball or soccer, or do gymnastics. Kids with flat feet, high arches, short leg syndrome, over-pronation (feet that roll inward when they walk) or who are overweight or obese also have an increased risk. Causes During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics. Symptoms The most prominent symptom of Sever's disease is heel pain which is usually aggravated by physical activity such as walking, running or jumping. The pain is localised to the posterior and plantar side of the heel over the calcaneal apophysis. Sometimes, the pain may be so severe that it may cause limping and interfere with physical performance in sports. External appearance of the heel is almost always normal, and signs of local disease such as edema, erythema (redness) are absent. The main diagnostic tool is pain on medial- lateral compression of the calcaneus in the area of growth plate, so called squeeze test. Foot radiographs are usually normal. Therefore the diagnosis of Sever's disease is primarily clinical. Diagnosis Sever's disease is based on the symptoms reported. To confirm the diagnosis, the clinician will examine the heels and ask about the child's activity level and participation in sports. They may also squeeze the back part of the heel from both sides at the same time to see if doing so causes pain and also ask the child to stand on tiptoes to see if that position causes pain. There may be tightness in the calf muscle, which contributes to tension on the heel. Symptoms are usually worse during or after activity and get better with rest. X-rays generally are not that helpful in diagnosing Sever's disease, but they may be ordered to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray. Non Surgical Treatment If your child have Sever's disease, the following is suggested, cut back on sporting activities, don't stop, just reduce the amount until symptoms improve (if the condition has been present for a while, a total break from sport may be needed later) avoid going barefoot, a soft cushioning heel raise is really important (this reduces the pull from the calf muscles on the growth plate and increases the shock absorption, so the growth plate is not knocked around as much). Stretch the calf muscles, provided the stretch does not cause pain in the area of the growth plate). The use of an ice pack after activity for 20mins is often useful for calcaneal apophysitis - this should be repeated 2 to 3 times a day. Prevention After the painful symptoms of Sever's disease have gone away, it is important to continue stretching the heel, particularly before a vigorous exercise, and wearing good supportive shoes fitted with children's arch supports. This will prevent heel pain recurrence until the child's heel is fully developed and less prone to injury.
Overview
 The exact number of people who develop Achilles tendon injury is not known, because many people with mild tendonitis or partial tear do not seek medical help. It is believed to be more common in men but with the recent participation of women in athletics, the incidence of Achilles tendon injury is also increasing in this population. Overall, injury to the Achilles tendon is by far most common in the athlete/active individual. The exact number of people who develop Achilles tendon injury is not known, because many people with mild tendonitis or partial tear do not seek medical help. It is believed to be more common in men but with the recent participation of women in athletics, the incidence of Achilles tendon injury is also increasing in this population. Overall, injury to the Achilles tendon is by far most common in the athlete/active individual.Causes There are a number of factors that can increase the risk of an Achilles tendon rupture, which include the following. You?re most likely to rupture your Achilles tendon during sports that involve bursts of jumping, pivoting and running, such as football or tennis. Your Achilles tendon becomes less flexible and less able to absorb repeated stresses, for example of running, as you get older. Small tears can develop in the fibres of the tendon and it may eventually completely tear. There is a very small risk of an Achilles tendon rupture if you have Achilles tendinopathy (also called Achilles tendinitis). This is where your tendon breaks down, which causes pain and stiffness in your Achilles tendon, both when you exercise and afterwards. If you take quinolone antibiotics and corticosteroid medicines, it can increase your risk of an Achilles tendon injury, particularly if you take them together. The exact reasons for this aren't fully understood at present. Symptoms A sudden and severe pain may be felt at the back of the ankle or calf, often described as "being hit by a rock or shot" or "like someone stepped onto the back of my ankle." The sound of a loud pop or snap may be reported. A gap or depression may be felt and seen in the tendon about 2 inches above the heel bone. Initial pain, swelling, and stiffness may be followed by bruising and weakness. The pain may decrease quickly, and smaller tendons may retain the ability to point the toes. Without the Achilles tendon, though, this would be very difficult. Standing on tiptoe and pushing off when walking will be impossible. A complete tear is more common than a partial tear. Diagnosis A detailed history, and examination by an appropriately qualified health professional, will allow a diagnosis to be made. An ultrasound or MRI scan can confirm the diagnosis. Other causes of symptoms in the area, such as those referred from the lumbar spine and local infection, should be excluded. Non Surgical Treatment The best treatment for a ruptured Achilles tendon often depends on your age, activity level and the severity of your injury. In general, younger and more active people often choose surgery to repair a completely ruptured Achilles tendon while older people are more likely to opt for nonsurgical treatment. Recent studies, however, have shown fairly equal effectiveness of both operative and nonoperative management. Nonsurgical treatment. This approach typically involves wearing a cast or walking boot with wedges to elevate your heel; this allows the ends of your torn tendon to heal. This method can be effective, and it avoids the risks, such as infection, associated with surgery. However, the likelihood of re-rupture may be higher with a nonsurgical approach, and recovery can take longer. If re-rupture occurs, surgical repair may be more difficult. 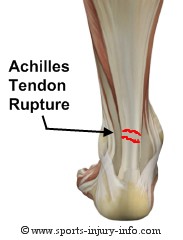 Surgical Treatment Surgical techniques for rupture repair are varied but usually involve reapproximation of the torn ends of the Achilles tendon, sometimes reinforced by the gastrocsoleus aponeurosis or plantaris tendon. Open reconstruction is undertaken using a medial longitudinal approach. Studies indicate that patients who undergo percutaneous, rather than an open, Achilles tendon rupture repair have a minimal rate of infection but a high rate of sural nerve entrapment (16.7% of treated cases). Prevention Good flexibility of the calf muscles plays an essential role in the prevention of Achilles tendon injuries. It is also important to include balance and stability work as part of the training programme. This should include work for the deep-seated abdominal muscles and for the muscles that control the hip. This might at first appear odd, given the fact that the Achilles are a good distance from these areas, but developing strength and control in this area (core stability) can boost control at the knee and ankle joints. Training errors should be avoided. The volume, intensity and frequency of training should be monitored carefully, and gradually progressed, particularly when introducing new modes of training to the programme. Abrupt changes in training load are the primary cause of Achilles tendinopathy.
Overview
Posterior tibial tendon dysfunction is one of several terms to describe a painful, progressive flatfoot deformity in adults. Other terms include posterior tibial tendon insufficiency and adult acquired flatfoot. The term adult acquired flatfoot is more appropriate because it allows a broader recognition of causative factors, not only limited to the posterior tibial tendon, an event where the posterior tibial tendon looses strength and function. The adult acquired flatfoot is a progressive, symptomatic (painful) deformity resulting from gradual stretch (attenuation) of the tibialis posterior tendon as well as the ligaments that support the arch of the foot.  Causes As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem. Symptoms Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot. Diagnosis In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot. Non surgical Treatment There are many non-surgical options for the flatfoot. Orthotics, non-custom braces, shoe gear changes and custom braces are all options for treatment. A course of physical therapy may be prescribed if tendon inflammation is part of the problem. Many people are successfully treated with non-surgical alternatives.  Surgical Treatment A new type of surgery has been developed in which surgeons can re-construct the flat foot deformity and also the deltoid ligament using a tendon called the peroneus longus. A person is able to function fully without use of the peroneus longus but they can also be taken from deceased donors if needed. The new surgery was performed on four men and one woman. An improved alignment of the ankle was still evident nine years later, and all had good mobility 8 to 10 years after the surgery. None had developed arthritis. |
